Lesson 2: Practical Management of Infant Feedings
2.2 Enteral Nutrition – Human Milk
The importance of nutrition for the preterm infants has been already discussed earlier in this module. The nutritional management aim in the NICU is to achieve growth similar to intrauterine fetal growth and development. Postnatal undernutrition is the main cause of postnatal growth restriction (PNGR) in preterm infants during their first weeks of life (Senterre 2014).
Enteral nutrition can be challenging in the preterm infant, mainly in those VLBW and ELBW infants. The risk of NEC and suspicion of feeding intolerance are the two main problems causing a delay in the preterm full enteral feeding in the NICU. Slow advancement of enteral feedings caused mainly by fear of these mentioned problems may lead to gastrointestinal mucosal atrophy (including increased permeability, decrease in mucosa regeneration capability, and reduced production of protective mucus), gastrointestinal dysfunction finally leading to feeding intolerance, and increased risk of NEC (Senterre 2014). Refer to Unit 1 Lesson 2.6 for further discussion in this subject.
Human Milk
Human milk (HM) is the enteral nutrition feeding choice for preterm infants (Ziegler 2014). HM provides the preterm infant with:
• Nutrients needed for growth and development
• Support and complements the developing immune system
In the HM, many bioactive components have been identified. Please refer to table 4 for a list of non-nutritive components of the human milk.
Table 4. Anti-infectious and other bioactive substances and cells in human milk.
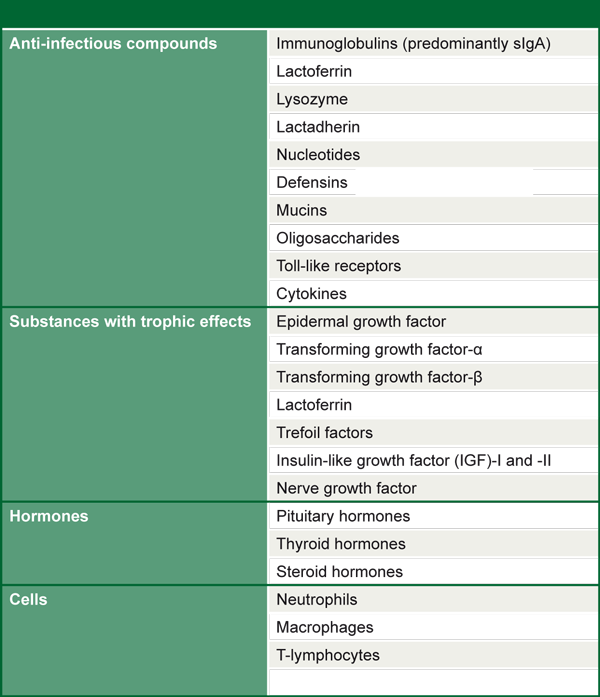
Source: Ziegler 2014, reprinted with kind permission of S. Karger AG, Switzerland
These components give the HM immune protection, exerting anti-inflammatory and anti-microbial functions. Oligosaccharides, which are present in large amounts in the HM, promote proliferation of healthy microbiota and reduce growth of pathogenic bacteria. As seen in Lesson 2.6 (unit 1), clinical studies have shown that the use of human milk is associated with the reduced risk of NEC and bacterial sepsis. The HM protective effect against sepsis has been shown to be dose-dependent (Patel et al. 2013). NEC prevention by the use of human milk is also associated with dosage. During the first two weeks of life, an increase of HM intake of 100 ml/kg decreases the risk of NEC by a factor of 0.87 (Meinzen-Derr et al. 2009).
Human milk also facilitates maturation of the preterm infant gastrointestinal tract, its use correlates to smaller gastric residuals (sign of an improved feeding "tolerance”), lower prevalence of abdominal distension and lower intestinal permeability (Ziegler 2014).
Other advantages of HM (Senterre 2014):
• Improvement in the mother-infant bonding;
• Reduction of the chance of hospital readmission due to illness after discharge;
• Reduction of severity of retinopathy of prematurity;
• Lower risk of development of metabolic syndrome later in life;
• Improved long-term neurodevelopmental scores.

Although HM is the recommended nutrition source in the NICU, breastfeeding may be challenging. Health care providers should encourage breastfeeding and provide parents with information in the benefits of human milk to the preterm infant. Mothers should be supported and encouraged to express human milk. Double electric breast pumps are normally recommended.
Nutritional requirements for the preterm infants are strictly correlated to body weight:
" ... protein needs are highest in the least mature and smallest infants and decrease with increasing body weight, whereas energy needs increase with increasing body weight due to increasing energy deposition in the form of fat. (Ziegler 2014)”.
Please refer to table 5.
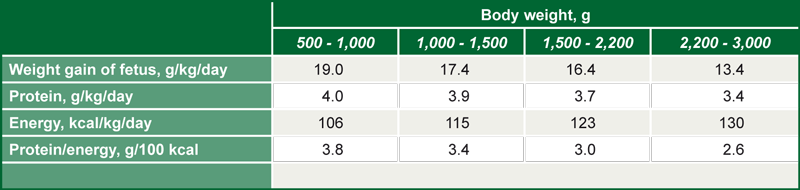
Source. Ziegler 2014, reprinted with permission of S. Karger AG, Switzerland
Based on current knowledge, it is clear that HM is the choice for enteral feeding in the preterm infant. However, most human milks alone will not supply adequately proteins, energy and other nutrients to support growth in the preterm infant. For that reason, human milk must be fortified to be able to provide all nutrients and energy necessary. In table 6, the nutrient requirements of ELBW and the typical composition of human milk with or without fortification are shown. Human milk will also not provide enough amounts of many vitamins for preterm infants, therefore supplementation must be carried out. In vitamin deficient mothers, maternal vitamin supplementation will increase the levels of the vitamins in the milk. However, for many vitamins, such as vitamin A, D or C, maternal supplementation will not be enough for preterm supply and use of fortifiers with vitamins supplementation should be used (Leaf & Lansdowne 2014).

Source. Ziegler 2014, reprinted with permission of S. Karger AG, Switzerland
Human milk fortifiers will be further discussed in lesson 2.4 of this unit.
Donor human milk
Donor human milk is a valuable resource for premature infants whose mothers are unable to provide an adequate supply of milk to their infants. Donor human milk banks follow guidelines and rules in how milk should be collected and stored. Human milk (HM) donors are carefully screened for infections (such as HIV, hepatitis, CMV) and risk of toxic contamination (use of medicines, recreational drugs, alcohol, tobacco). Donor HM is normally pasteurized (62.5°C for 30 minutes) to reduce the risk of exogenous contamination. The use of donor HM versus preterm formula in VLBW infants have been investigated in a number of studies. The risk of NEC was particularly reduced in infants receiving donor HM (Senterre 2014). Preterm infant formulas will be further discussed in lesson 2.5 of this unit.