Lesson 2: Practical Management of Infant Feedings
2.3 Practical Management of Enteral Nutrition
Initiation of Enteral Nutrition
Considerable debate exists on when and how to start enteral feeds in preterm infants. The introduction of enteral feeds in preterm infants is often delayed for days to over a week after birth due to concerns about gut immaturity and risk of developing NEC. Please refer to Unit 1 Lesson 2.6 "Necrotizing enterocolitis” in this module. As already discussed earlier, over caution in the use of the premature infant's gastrointestinal (GI) tract, however, can be harmful, leading to GI mucosal atrophy and changes in the bacterial milieu which may actually predispose an infant to NEC and sepsis (Senterre 2014). A systematic review published in 2014 found that delaying enteral feeds for more than four days after birth did not reduce the incidence of NEC or death but did lead to a 2-4 day delay in the establishment of full enteral feeds (Morgan et al. 2014a). It is important to note that a delay in the establishment of full enteral feeds requires longer use of PN, which carries its own risks (See Lesson 2.1 of this Unit).
Feeds are often started at very low rates of less than or equal to 24 ml/kg/day. This is called minimal enteral feeding (MEF), also known as "trophic feeding” or "gut priming” (Senterre 2014). Delayed enteral feeding compared to MEF in the first week of the VLBW infant's life is associated with lower weight gain, lower head growth, higher incidence of nosocomial sepsis, longer PN, later full enteral feeding and later hospital discharge without showing any advantages (Senterre 2014). A systematic review of early MEF - defined as started within four days of birth - versus enteral fasting did not show any adverse effects or higher risk of NEC in trophic feeding (Morgan et al. 2013).
Feeding administration
Preterm infants generally require a feeding tube as they are unable to coordinate sucking, swallowing and breathing and thus risk aspiration if fed orally. Feeding tubes can be inserted via the mouth (orogastric tube) or nostril (nasogatric tube). A nasogastric tube is easier to secure than an orogastric one and will not be displaced by tongue movements. However, nasogastric tubes partially obstruct the nasal airway and may increase the work of breathing and thus increase overall energy expenditure (Senterre 2014). A Cochrane systematic review was not able to show a clear advantage of nasal or oral route placement (Watson & McGuire 2013a).
Optimal tube position has also been studied. Positioning the tube in the stomach is recommended over placement in the small bowel. Though inserting a feeding tube beyond the pyloric sphincter might theoretically reduce the risk of gastroesophageal reflux and aspiration pneumonia and possibly apneic and bradycardic events, study data suggest that this practice confers no benefits and increases the risk of gastrointestinal disturbance and mortality (Watson & McGuire 2013b). Thus, positioning the tube in the small bowel is not recommended.
Unfortunately, correct placement of the tube with its tip or side orifice in the body of the stomach can be challenging. A study by Quandt and colleagues showed that only 41% of tubes were correctly positioned when checked radiographically (the gold standard for checking tube placement, although ultrasound can also be used). A misplaced tube can lead to complications, such as gastroesophageal reflux, risk of pulmonary aspiration and injury of the gastroesophageal mucosa (Quandt et al. 2009).
Results published in 2012 from an international survey (Klingenberg et al. 2012) of neonatal care units in four geographic regions (UK/Ireland, Scandanavia, Australia and Canada) demonstrated that enteral feeds are administered to preterm infants in many different ways: as intermittent boluses given over minutes to hours at intervals ranging from 1 to 3 hours or as continuous feeds. Continuous feeding methods may improve feeding tolerance, decrease the stress and risk of reflux that could result from high-volume boluses, decrease the time to achieve full enteral feeding, and support linear growth in ELBW (Senterre 2014). However, no statistical differences were seen in time to achieve full enteral feeding, postnatal growth, hospitalization duration and NEC incidence, when comparing continuous and intermittent bolus feeding in a recent systematic review in VLBW infants (Premji & Chessell 2011).
Enteral Nutrition advancement
The optimal rate of enteral feed advancement has also been debated, with concerns for increasing the risk of NEC when feeds are advanced more than 15-20 ml/kg/day in infants born at <32 weeks or <1500g. Another recent systematic review, however, concluded that advancing feeds at the faster rate of 30-35 ml/kg/day not only did not increase the risk of NEC but also led to a more rapid return to birthweight and attainment of full enteral feeding. This review did not include large numbers of extremely premature or extremely low birthweight infants (Morgan et al. 2014b).
Feeding Tolerance
As feeds are advanced, the infant is usually assessed clinically for feeding intolerance. The more obvious indications of feeding intolerance include emesis, vomiting, severe abdominal distension. These findings in association with systemic symptoms such as hemodynamic instability, bradycardia or apnea are worrisome for NEC. Feeds may need to be interrupted or reduced, though they should be resumed as soon as severe pathology is ruled out. The differential diagnosis of feeding intolerance must be carefully considered. Of note, some degree of abdominal distention can occur with non-invasive ventilatory support (Senterre 2014).
Unfortunately, however, there is no validated method of testing feeding intolerance. Although aspiration of gastric residuals is commonly used as evaluation of GI tolerance, little (if any) clinical evidence indicates the usefulness of gastric residuals as predictive of feeding intolerance. Concern about gastric residuals may lead to unnecessary feeding interruptions and their routine assessment is being called into question (Torrazza et al. 2014).
Feeding Logistics
When planning a feeding strategy for the preterm infant, not only the nutrient composition should be taken in consideration. Feeding prescriptions should also take handling and feeding concentration into consideration - the latter depending on the physical and laboratorial conditions of the infant. When adding powdered or liquid human milk fortifiers, medications or other supplements to milk, or when reconstituting artificial preterm formula, neonatal care providers must pay some attention to the high osmolarity of the resulting feeds. Though concentrating feeds may be desirable as part of an effort to restrict fluids in infants with some medical conditions such as lung or heart disease, gastric emptying may be slowed in response to high osmolar loads (Senterre 2014).
Proper storage and handling of HM, donor human milk (DHM) and reconstituted preterm formula should be part of any NICU guidelines. The use of glass-fronted refrigerators, for example, should be discouraged since they expose the HM and formula to light, possibly causing oxidation (Senterre 2014).
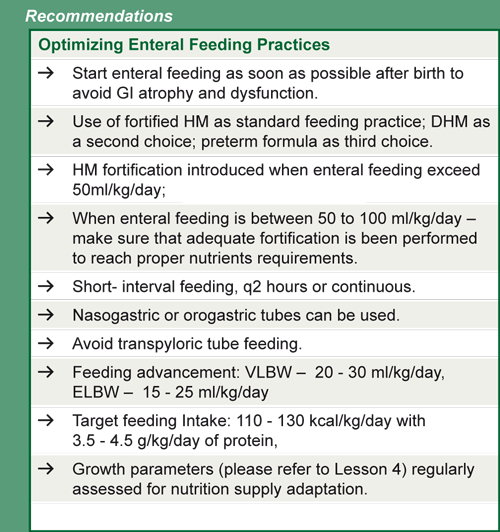
Please refer to Table 7 for a feeding strategy summary for VLBW and ELBW infants
Table 7. Reasonable strategy to optimize enteral feeding in ELBW (<1000g) and VLBW (1000-1499g) infants
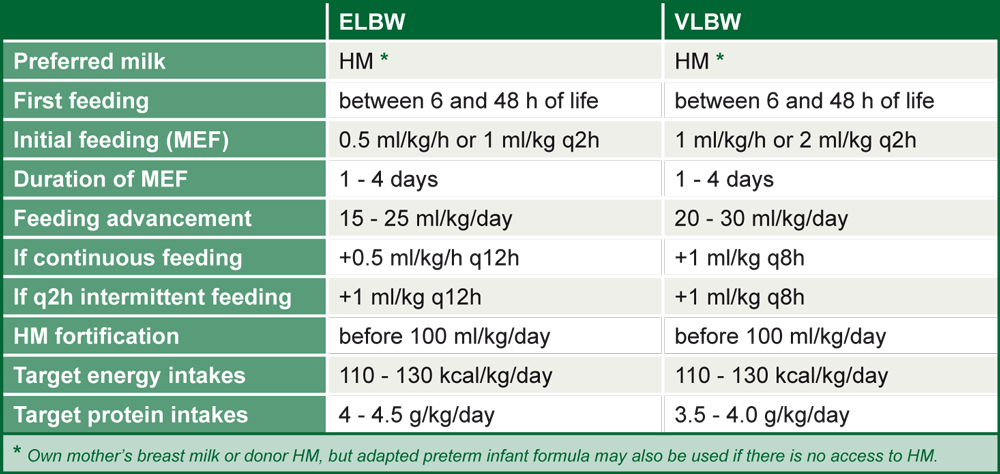
Source: Senterre 2014, reprinted with permission of S. Karger AG, Switzerland