Lesson 5: Preterm Infant Nutritional Management in Low-resource Settings
5.2 Enteral feeding of preterm infants in a resource-constrained setting
The initial management of VLBW infants in a resource-constrained facility may have to be done in a neonatal ward, since the availability of NICUs facilities in low-income countries is reduced. Ventilation support might not be available for all and nasal continuous positive airway pressure is widely used.
As in other settings, human milk is the enteral feeding choice also in low-resource countries. However, in some countries with high maternal HIV infection prevalence, the risk of transmission of HIV through expressed breast milk (EBM) has to be considered. Colostrum should be started soon after birth. As in resource-rich settings, expression of milk should begin as soon as possible after the delivery of a preterm infant. It is unlikely that breast pumps will be available in resource-limited settings. Moreover, their use is discouraged due to concerns of disease transmission (e.g. HIV, cytomegalovirus, Hepatitis B) with pump sharing (Murguia-Peniche & Kirsten 2014).

Source: Born to Soon (WHO et al. 2012)
The first drops of colostrum should be collected in a sterile spoon or syringe and given to the infant directly. This practice has been found safe even in very sick ELBW (Rodriguez et al. 2010; Seigel et al. 2013). Mothers must fully empty their breasts manually throughout the day (e.g. 8 to 21 times) to establish milk supply. If refrigerators or freezers are not available, milk can be stored up to 4 hours at room temperature. Otherwise, milk should be refrigerated immediately after expression for up to 96 hours at 4°C. If it will be stored for longer than 96 hours it should be frozen (Murguia-Peniche & Kirsten 2014).
In many resource-limited settings, maternal infection with HIV may be common. It is critical to document the HIV status of pregnant women in order to prevent vertical transmission to their infants at birth or through breastfeeding. Flash-heating pasteurization is a technique to reduce the risk of transmission of the HIV virus to the infant via expressed human milk. Women known to be HIV+ as well as women who do not wish to be tested should pasteurize their freshly expressed milk. Flash-heating pasteurization can be taught to new mothers, who then can carry out the procedure themselves. Freshly expressed human milk is placed into a sterile, heat-resistant container such as a glass jar and the sterilized lid is put on. This jar, in turn, is placed in a pot, which is then filled with enough water to reach 2 cm (about 2 fingers' breadth) above the level of the milk in the jar. The water is brought to a full or rolling boil over high heat. The jar is then removed and allowed to cool to room temperature. At that point the milk can be given directly to the infant or stored at room temperature in the jar for up to 24 hours. Alternatively, it may be refrigerated for up to 96 hours or frozen (Murguia-Peniche & Kirsten 2014).
A video showing the flash-heating process in human milk can be seen here.
Any neonatal facility handling milk from known or potentially HIV+ mothers must have a system for tracking the HIV status of each mother while maintaining confidentiality. Ideally, there should be separate refrigerators and freezers for storing the expressed milk from HIV+ and HIV- mothers. There must be a clear labeling system and protocols in place for verifying and cross-checking that the proper milk is given to each baby. Additionally, it is important to have a plan in place for post-exposure prophylaxis in case a baby inadvertently receives milk from an HIV+ mother (Murguia-Peniche & Kirsten 2014).

Source: Born to soon (WHO et al. 2012)
Donor human milk can also be used when the mother is not able to express or produce milk. Donor human milk is also pasteurized and should be provided from women who are healthy, non-smoking, non-users of recreational drugs and HIV, Hepatitis B, syphilis and CMV negative.
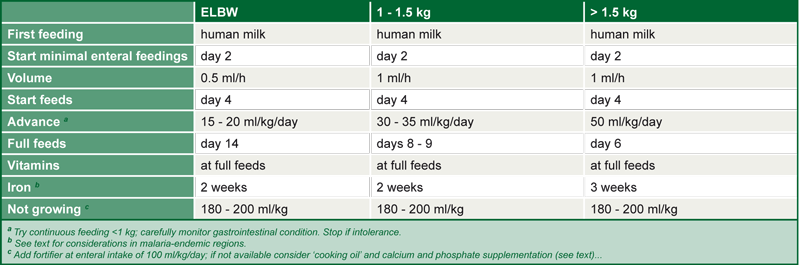
The enteral nutrition goal for preterm infants in resource-limited settings is to reach full enteral feeds of about 150 ml/kg of expressed human milk as soon as possible after birth. As in other settings, tube feedings will generally be necessary, depending on the degree of prematurity. As a recommendation, continuous tube feedings starting with 0.5 ml/h on day 1 in stable ELBW infants should be carried out, advancing the feeding volumes cautiously by 30 ml/kg/day. It may take a week for ELBW infants to reach full feeds. For VLBW and LBW infants, more rapid advancement of feeds is suggested (Murguia-Peniche & Kirsten 2014).
The protein and energy content of expressed milk will most likely be inadequate to support growth at a target rate of 15 g/kg/day. Feed volumes may have to be increased to 200-220 ml/kg/day, and given in frequent small portions to increase protein and energy intake. If available, HMFs are also recommended to increase intake of protein, calories, calcium, phosphate, vitamins and iron (Murguia-Peniche & Kirsten 2014). HMFs can be started when enteral intakes are tolerated. In ELBW it is suggested that fortifiers be started at half-strength for the first few days, then advanced to full strength (Murguia-Peniche & Kirsten 2014). Table 11 outlines approaches when HMFs are unavailable.
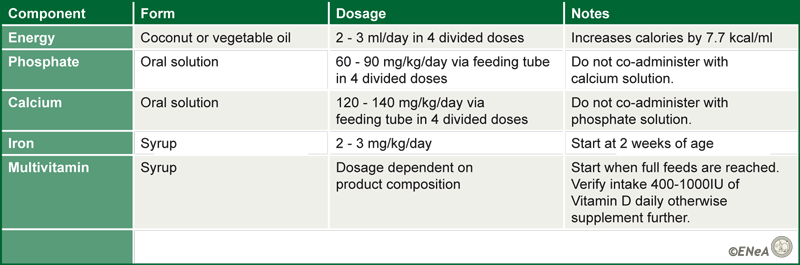
Source: ENeA own table. Data from Murguia-Peniche & Kirsten 2014
Source: Murguia-Peniche & Kirsten 2014; reprinted with permission of S. Karger AG; Switzerland
Table 13. Proposed strategy for feeding unstable preterm infants in low-resource settings
Source: Murguia-Peniche & Kirsten 2014; reprinted with permission of S. Karger AG; Switzerland