Lesson 6: Fluid and electrolyte requirements
6.1 Water Physiology
 Normal water homeostasis knowledge is essential for proper fluid management in the preterm infant. Circulation and metabolism can be highly compromised when not enough fluid is provided. On the other hand, oversupply should also be avoided, since too high intake has been linked to conditions such as patent ductus arteriosus and chronic lung disease (Fusch & Jochum 2014).
Normal water homeostasis knowledge is essential for proper fluid management in the preterm infant. Circulation and metabolism can be highly compromised when not enough fluid is provided. On the other hand, oversupply should also be avoided, since too high intake has been linked to conditions such as patent ductus arteriosus and chronic lung disease (Fusch & Jochum 2014).
Water is not distributed equally throughout the body. Fat mass is assumed to be water-free. Most of the body water is found in the lean tissue, therefore, lean body mass rather than total body mass correlates with total body water. At 24 weeks a fetus' body weight is about 90% water. By term it is 75% (Fomon et al. 1982; Widdowson 1981). This reflects, in part, the fetal body composition shift in the last weeks of gestation because the fetus accretes fat mass after 32 weeks (Friis-Hansen 1961). More information about body water compartments through life with age-related changes of total body water and its compartments, the intracellular and extracellular volume, from fetal life until adolescence, can be found in the historical paper by Friis-Hansen from 1961 (Friis-Hansen 1961) and also on figure 1 of Fusch & Jochum 2014.
Body Water Compartments
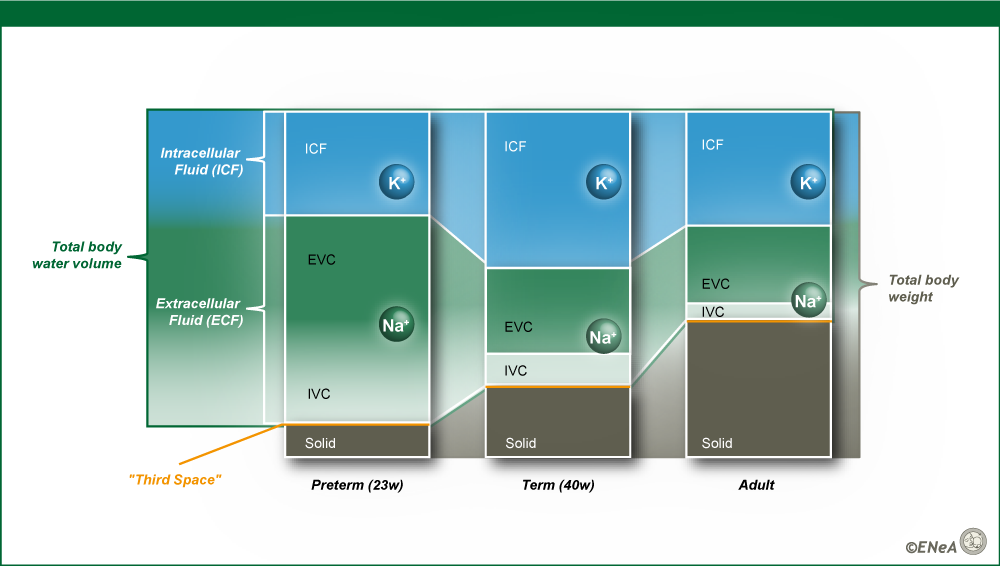
Figure 7. Body water compartments in preterm infant, term infant and adult.
Typical solid and body-water distribution in preterm and term infants, and adults (to scale). Solid contribution varies between 5-8% (preterm), 10-25% (term) and 8-50% (adults). ICF contribution is generally 30%, 45%, and 35% respectively.
"Third space” represents free fluid in physiological conditions (e.g urine, cerebrospinal fluid) and pathological conditions (e.g ascites, pleural effusions). Potassium (K) is the leading ion in the intracellular fluid (ICF) and sodium (Na) is the leading ion in the extracellular fluid (ECF). EVC: Extravascular fluid, IVC: Intravascular fluid.
Source: ENeA own