Lesson 6: Fluid and electrolyte requirements
6.2 Homeostasis of body water
Extracellular Fluid (ECF) regulates water metabolism (Figure 8). This regulation is dependent of intake, absorption and excretion of fluids and it is done through the intravascular compartment (IVC). It targets the following:
- Maintenance of blood pressure and adequate circulation (Friis-Hansen 1961)
- Maintenance of the ECF compartment osmolality within 280-290 mosm (3% of the set point) (Andersson 1977).
To be able to regulate and promote homeostasis, the body signalizes and changes the water intake through:
- Thirst (although not in the infant, since water intake in controlled by others)
- Vascular tone, heart rate and contractility,
- Renal excretion of water and electrolytes. The whole system is tightly regulated by hormonal action (renin-angiotensin-aldosterone system, arginine vasopressin and atrial natriuretic peptide) (Fusch & Jochum 2014)
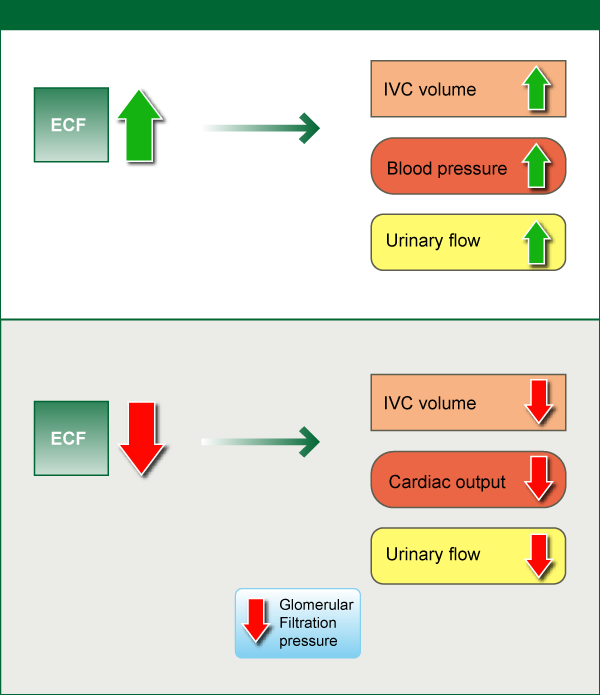
Figure 8. Fluid homeostasis controlled by the ECF (Extracellular Fluid) compartment under healthy conditions. IVC (intravascular compartment)
Source: ENeA own graph
Regulation of ICF and ECF - The Na+/K+-ATPase pump is the main regulator of the ICF:ECF ratio in the body (figure 9). As a consequence, the ICF is shielded from direct interface with the external environment, avoiding drastic changes in its volume and concentration.
Regulation of IVF and EVF- The EVF:IVF ratio in normal conditions is dependent on blood and oncotic-hydrostatic pressure and permeability of the capillary wall. Preterm infants present an EVF:IVF ratio higher than term infants and adults (Friis-Hansen 1961). Although the permeability of the capillary wall does not seem to change with age, the oncotic-hydrostatic pressure appears to be lower in neonates than in adults, explaining the changes in the ratio throughout life.
Fetal Water and Electrolyte Metabolism: Water transfer is made through the placenta from mother to fetus. Electrolytes are actively transferred to the fetus through the placenta leading to equilibrium between mother and fetus. The electrolyte concentration in the fetus depends upon the maternal plasma concentration. At 5 weeks of gestational age, the fetus starts with urine production. At 20 weeks, around 4.5 ml/kg/h of urine is produced, going up to 8-15 ml/kg/h at term.
Water input (see also figure 9 on the next page):
- water given orally and parenterally,
- metabolic water generated from the oxidation of fats and carbohydrates (and from proteins when non-protein energy supply is inadequate). Oxidation of carbohydrates can produce 0.6 ml of water per gram, while fats produce 1 ml H2O/g. Thus, a healthy infant produces daily 5-15 ml/kg of metabolic water. Stress causing an increase in metabolism can elevate this metabolic water production up to 20ml/kg/day.
Water output (postnatal)
- Insensible water loss via skin (dependent from gestational and postnatal age and environment). Losses through immature skin are highest in the smallest infants due to their high surface to volume ratio.
- Water loss via respiration, one third of net insensible water loss is done through evaporation from the upper respiratory tract. Premature infants lose more water (0.8-0.9 ml/kg/h) than term infants (0.5 ml/kg/h) due to their higher respiratory rate. However, evaporation and water loss can be dramatically reduced if the infant is kept at 37°C and 85-100% relative humidity.
- By urine production.
- Fecal losses, which are negligible in preterm infants that have not yet initiated enteral feeding. 5-10 ml/kg/day of water will be lost in stools once full enteral feeding is established.
- Growth, water is also needed for growth.