Lesson 6: Fluid and electrolyte requirements
6.3 Metabolism of Sodium, Potassium and Chlorine
Intake:
- No endogenous production, totally dependent of exogenous source,
- Enteral intake and parenteral intake in newborns totally dependent of administration.
Output:
- Sweat and perspiration,
- Urine, which is actively regulated. Urinary excretion of electrolytes is dependent of intake and gestational and postnatal age (maturity of the urinary system). In a normohydrated neonate, urinary concentration of Na+ is about 20-40 mmol/l and 10-30 mmol/l for K+ (Fusch & Jochum 2014). Urinary excretion of electrolytes is fairly constant throughout the day, and it is, within physiological conditions, independent of water regulation.
- Feces. Na+ losses in stools is dependent on age. Preterm infants tend to lose more Na+ (0.1 mmol/kg/day) than term infants (0.002 mmol/Kg/day). K+ fecal losses are generally twice as high as Na+ but are not related to gestational age.
- Additional losses occur in special situations: bowel obstruction, ileostoma, pleural effusions, peritoneal drainage, and repeated cerebral spinal fluid drainage. It is advisable, whenever possible, to measure electrolyte concentration in such fluids for loss quantification.
- Growth: accretion of lean body tissue requires electrolytes (being stored in the accreted tissue) and it has been shown that growth and weight gain are slowed in preterm infants when insufficient sodium is available (Bower et al. 1988; Haycock 1993).
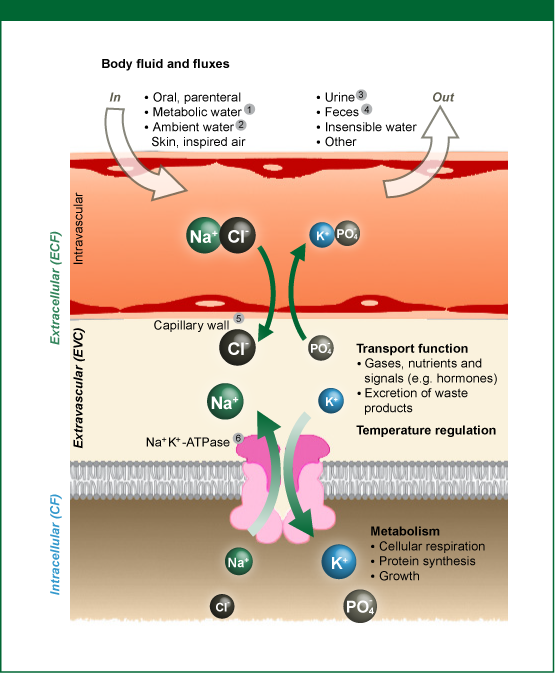
Figure 9: Water and electrolyte fluxes between body water compartments.
1) metabolic water production depending on exact intake of carbohydrates, protein and fat (approx. 15 ml/kg/day),
2) input via skin and inspired air,
3) volume depending upon need for excretion of fixed acids and urea and desired urine osmolarity,
4) fecal water losses: quantities are negligibly small in healthy subjects, but considerable in diarrhea and/or in presence of ileostoma (e.g. NEC surgery),
5) oncotic pressure,
6) activity of Na+ /K+ -ATPase defines the long-term ratio of ECF/ICF; short-term changes are subject to short-term variation of ECV; content of water and electro-/osmolytes: any change in either ICV or ECV osmolarity will result in movement of water into the compartment with the higher osmolarity.
Source: Fusch & Jochum 2014, reprinted with permission of S Karger AG, Switzerland