Lesson 9: Vitamins
9.2.1 Fat-soluble Vitamins – Vitamin A
 Vitamin A is a sub-class of lipid-soluble compounds chemically defined as retinoids. They consist of four isoprenoid units joined in a head to tail fashion. Vitamin A has two main forms:
Vitamin A is a sub-class of lipid-soluble compounds chemically defined as retinoids. They consist of four isoprenoid units joined in a head to tail fashion. Vitamin A has two main forms:
- Provitamin A carotenoids, including ß-carotene and others. Carotenoids are found in green leafy vegetables, sweet potatoes and carrots. ß-carotene is the only one that is metabolized by mammals into vitamin A.
- Preformed vitamin A, including retinol, retinoic acids, and others. The most active form of vitamin A, retinol, is mostly found in animal sources (egg yolk, liver, fish oils).
Vitamin A has been found to have an essential role in vision, reproduction, healing processes, growth, cell differentiation and in the immune system. In the fetus, vitamin A is required for lung cell differentiation and surfactant production (Mactier & Weaver 2005). Vitamin A is also important for fetal lung development. Retinoic acid is responsible for surfactant proteins regulation through the retinoic acid nuclear receptor. Therefore, vitamin A deficiency in the preterm infant might contribute to BPD and increases the risk of respiratory tract infections (Leaf & Lansdowne 2014).
Premature infants have lower vitamin A concentration in cord blood than term infants. They also present with lower vitamin A storage in liver, since most of the vitamin A accumulation occurs after the 26th week of gestation. On top of that, they also have lower concentrations of retinol-binding protein (RBP) in the plasma, necessary for retinol transportation to target organs (figure 11).
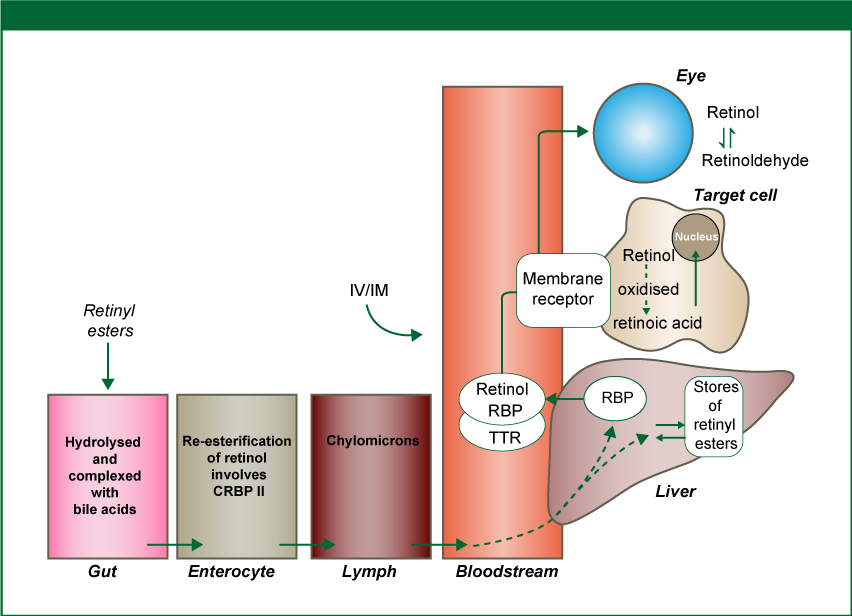
Figure 11. Uptake and metabolism of vitamin A.
CRBP II = Cellular retinol-binding protein type 2; IV = intravenous; IM = intramuscular; RBP = retinol-binding protein; TTR = transthyretin.
Source: adapted from Leaf & Lansdowne 2014; reprinted with permission of S. Karger AG, Switzerland
Vitamin A plasma concentration of <200 µg/l (0.70 µmol/l) in the preterm infant is considered deficient, and when these values are lower than 100 µg/l (0.35 µmol/l) severe deficiency is diagnosed with absence of liver storage (Greer 2005). Vitamin A deficiency has been associated in both humans and animal models with chronic lung disease of prematurity. A recent Cochrane review that evaluated the administration of relatively high doses of intramuscular Vitamin A during the early weeks of life of the most vulnerable preterm infants, concluded that although modest, a significant improvement in respiratory outcome was seen (Darlow & Graham 2011). The same review also showed a reduction in retinopathy of prematurity, although not significant. They also describe a non- significant difference in the incidence of intravascular hemorrhage, no effect in the closure of patent ductus arteriosus and a non-significant reduction in culture-positive nosocomial sepsis (Darlow & Graham 2011).