Lesson 2: Why Do Some People Get Celiac Disease and Most Don't- Although They All Eat Gluten?
2.1 The role of genes
There is a certain inherited (=genetic) predisposition for the development of celiac disease. The main celiac disease risk gene variants are called HLA-DQ2 and HLA-DQ8 and they are found in about 1 of 3 individuals (30-40%) in the European population (see figure 4). Although these risk variants are so frequent, only 1% of the whole population will finally get celiac disease. People who do not carry HLA-DQ2 and/or HLA-DQ8 are not at risk of developing celiac disease.
Imagine a village with a population of 1000 inhabitants (figure 4). Of these, around 350 carry the celiac disease risk gene variants HLA-DQ2/DQ8 which are the basis for celiac disease development. In total, about 10 of them have already got celiac disease or will develop it. This means 1% of the whole population (respectively 3% of the subgroup with the risk genes) are affected. Two thirds of them are female.
Among the 10 inhabitants with celiac disease, only 1-2 are medically diagnosed. The remainder may have symptoms that have not been diagnosed as caused by celiac disease or may experience no obvious symptoms at all.
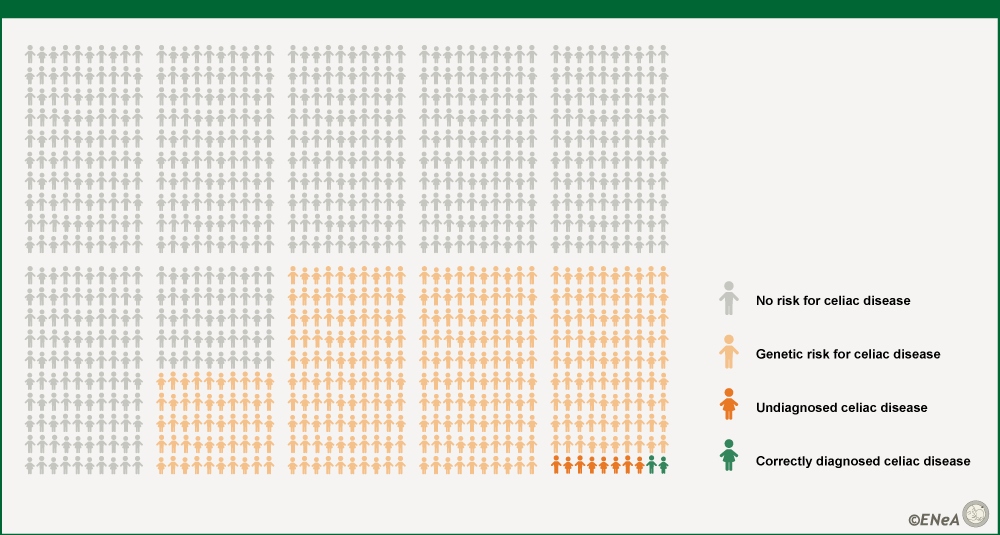
Figure 4: Prevalence of HLA-DQ2/DQ8 and celiac disease
Source: ENeA own
There are many other genes involved in celiac disease course and development (called non-HLA-genes). But on their own they contribute only slightly to the overall risk. The HLA-DQ2 and HLA-DQ8 genes are the most important genes in the development of the disease. However, as only very few of those individuals with HLA-DQ2/DQ8 finally get celiac disease, we know that there must be environmental processes involved in disease development (Unit 1, lesson 2).
You'd like to learn more details about the genetics of celiac disease? Click here to get some further information!
Familial risk
As a consequence of the genetic predisposition, celiac disease is more common among family members. About 10% (1 in 10) of close family members (parents, siblings or children of people with celiac disease) are also affected by celiac disease.
Studies in twins show very nicely how important the genes are for the development of celiac disease. Monozygotic twins have exactly the same copy of genes - in other words, they are natural clones. If a monozygotic twin is diagnosed for celiac disease, the probability for the other twin is 75% (3 in 4 monozygotic twins will get the disease) (see figure 5). In dizygotic twins, which are genetically not more or less similar than other siblings, it's only about 10-20% (1 or 2 in 10, as for all other first degree relatives).
However, a quarter of the monozygotic twins do not develop the disease despite having exactly the same genes as their twin sibling with celiac disease. This means celiac disease has indeed a strong inheritance background but does not follow a simple genetic trait.
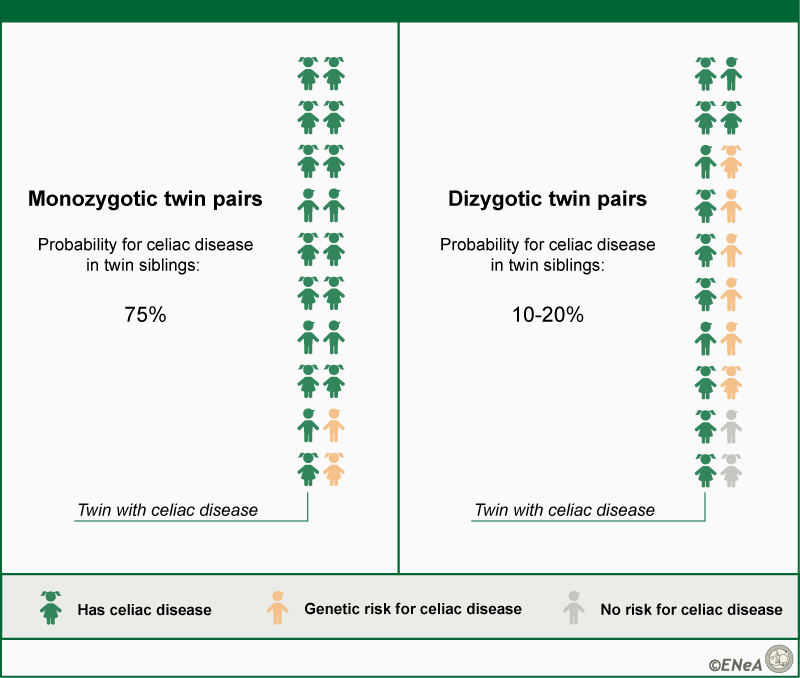
Figure 5: Twin studies show the strong genetic component of celiac disease
When you find 10 monozygotic twin pairs with celiac disease in one of the twins, the probability that the other twin sibling has celiac disease or will develop it is 75% (7-8 in 10). This means celiac disease is not an inherited disease as such, as not all monozygotic twin siblings get it. Dizygotic twins are however not more similar than other siblings. When you have 10 dizygotic twin pairs with celiac disease in one of the twins, the probability for the other twin to develop celiac disease is only 10-20% (1 or 2 of 10). The others may or may not carry the risk genes and do not get celiac disease.
Source: ENeA own
Because of their increased risk, first-degree relatives of a celiac disease patient may be actively investigated for the presence of the HLA-DQ2 and HLA-DQ8 genes. If they do not show these genetic variants, no further investigations are needed. If they carry one or more of the HLA risk markers they should be tested for celiac disease with specific blood tests. For further information on HLA-testing and celiac disease diagnosis see Unit 2, lesson 1.