Lesson 2: Why Do Some People Get Celiac Disease and Most Don't- Although They All Eat Gluten?
2.2 Other high-risk groups
Apart from family members, there is an increased risk of celiac disease among other specific groups of individuals.
Celiac disease and other autoimmune diseases
As you have already learned, celiac disease belongs to the group of autoimmune diseases. This means that the body’s immune system reacts against its own tissue. Celiac disease is also genetically “linked” with other autoimmune diseases that affect other organs. The following autoimmune diseases belong to this group:
• autoimmune thyroid disease
• type 1 diabetes mellitus
• autoimmune liver disorders
• juvenile idiopathic arthritis
• autoimmune skin disorders (e.g. vitiligo, psoriasis)
About 1 in 4 patients with celiac disease will develop one of these other autoimmune diseases in their lifetime. Vice versa, patients with one of these autoimmune diseases also have a higher risk to develop celiac disease.
Celiac disease and selective immunoglobulin A (IgA) deficiency
The body’s immune system is very complex and there are many inherited causes that can be responsible for it not working properly. The most common immune deficiency in the general population (1 in 600) is selective immunoglobulin A (IgA) deficiency (IgA deficiency). Immunoglobulins (Ig) are proteins which are also called antibodies. They are produced by the immune system as weapons against harmful invaders such as bacteria and viruses. There are five different classes. The class of IgA immunoglobulins are primarily present in the mucosal surfaces such as the gastrointestinal tract. In individuals with selective IgA deficiency, the production of these IgA antibodies is very low or completely missing. Nevertheless, the majority of affected individuals is never diagnosed and remains healthy. They have a tendency though for acquiring infectious diseases. However, compared to the general population, individuals with IgA deficiency are at increased risk for developing celiac disease. Vice versa, IgA deficiency is also more frequent among celiac disease patients.
Celiac disease and chromosomal abnormalities
Usually,
the whole genetic information of every individual is packed in 46
chromosomes that carry all information for the “construction plan” of
our body. Each chromosome is present as a copy, so we actually have 23
pairs of chromosomes (see figure 7). One of these pairs is our sex
chromosomes - in women there are two copies of chromosome X, while men
have one X and one Y chromosome. In individuals with chromosomal
abnormalities, there may be only 45 or even 47 chromosomes or parts of
chromosomes are missing or doubled. In some of these conditions, celiac
disease occurs more frequently. Therefore, testing for celiac disease or
the HLA-markers is useful in some of the chromosomal disorders.
Individuals
with Down syndrome have three copies of chromosome 21 rather than
two. They are five times more likely to develop celiac disease compared
to the general population, that is 5% compared to 1% risk. A similarly
increased risk exists for females with Turner syndrome who only have one
copy of the sex chromosome X instead of two. The risk for individuals
with Williams-Beuren syndrome is even greater with a 9-fold increased
risk.
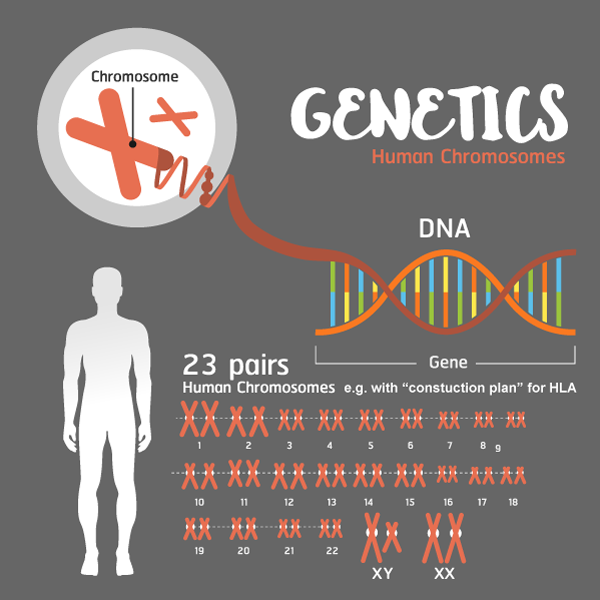
Figure 7: The genetic code of our body
Chromosomes are thread-like structures located inside the nucleus of each cell in our body. Chromosomes contain the genetic information written in a DNA molecule. These contain the “construction plan” for every structure in our body. Each chromosome is present as a copy, so we actually have 23 pairs of chromosomes, one pair thereof is our sex chromosomes.
Source: modified from Shutterstock (ID 648893830)
What should individuals do if they belong to one of these risk groups?
Testing for the celiac disease risk genes HLA-DQ2/DQ8 may be useful (see Unit 2, lesson 1).
If the result is negative (no HLA-DQ2/DQ8 variants present), there is no risk to develop celiac disease and no further tests are needed.
If the genetic risk is confirmed or unknown, routine screening for celiac antibodies is worthwhile. Children in these risk groups should be tested every one to two years for celiac disease antibodies until adolescence (12 years) or if they experience relevant symptoms (learn more in Unit 2, lesson 1). If no antibody tests were done in childhood and adolescence in an already adult individual, this should be done at least once or immediately if relevant symptoms are present.
However, a person positive for HLA-DQ2 and/or HLA-DQ8 should not be worried too much and always keep in mind that the chance of not developing celiac disease is much higher than the chance of developing it!