Lesson 8: Complementary Feeding in Developing Countries
8.3 Stunting

Photo by Mercedes de Onis,
Dept. of Nutrition, WHO;
reprinted with permission of WHO
The child on the left is
26 months old and the one
on the right is 52 months old.
Stunting is a type of growth faltering. Children with linear growth retardation are those whose height-for-age is less than 2 standard deviations below the WHO standard (Caulfield et al. 2006). Evidence does not support the assumption that children of certain racial and ethnic groups are naturally short (Lutter et al. 2011). Modern research supports the assertion that all healthy children can reach their growth potential if recommendations for adequate nutrition, medicine and child care are followed (Lutter et al. 2011).
Although many children are not classified as being stunted until preschool age, the process of becoming stunted actually begins before a child is born as a result of poor nutrition during pregnancy and is often regarded as an intergenerational problem since stunted women tend to give birth to stunted offspring (Dewey & Begum 2011). Stunting is a result of insufficient nutrient status caused by inadequate dietary intakes, recurrent infectious diseases, reduction of appetite from these conditions, increased metabolic requirements or nutrient losses. It has been demonstrated that dietary diversity correlates with height-for-age z scores (Arimond & Ruehl 2004).
Ninety percent of all childhood stunting worldwide is found in only 36 countries (Black et al. 2008). In fact, stunting affects 25-30% of all children in the developing world (Engle et al. 2009). Figure 10 shows the percent of children less than five years old that are stunted and their respective regions.
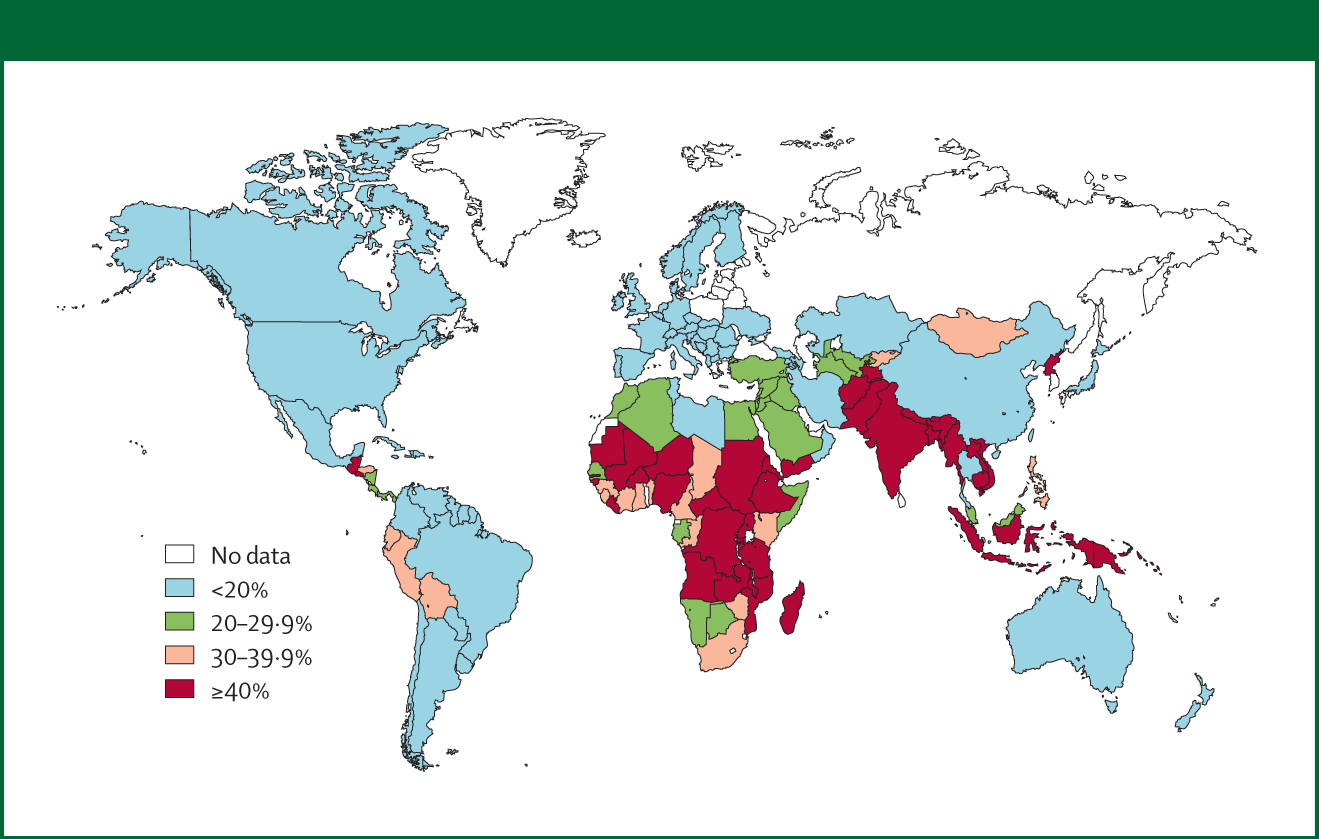
Figure 10: Prevalence of stunting in children under 5 years
Source: Black et al. 2008, reprinted from The Lancet with permission from Elsevier
A Lancet series on child development recognized tackling stunting, iron and iodine deficiencies amongst the top four most effective early childhood development interventions (Engle et al. 2007). It is known that stunting in early childhood is caused by malnutrition and infection rather than by genetic differences across countries (Grantham-McGregor 2007). Faltering may begin as early as in utero and is pronounced in the first 12-18 months but could continue longer (Grantham-McGregor 2007). In low- and middle-income countries, infants are at the greatest risk of malnutrition and stunting during the complementary feeding period (Przyrembel 2012). Therefore, this period is considered a critical window for prevention of growth faltering (Dewey & Adu-Afarwuah 2008). While some catch-up growth might take place, most stunted children remain stunted throughout their lives (Grantham-McGregor 2007) and it is very difficult to reverse the impact of stunting after two years of age (Dewey & Adu-Afarwuah 2008). In developing countries, the age at introduction of complementary foods may prevent growth faltering when breastfeeding is continued and hygiene and composition of the complementary food are adequate (Przyrembel 2012).
In an article published in the Lancet in 2008, authors wrote about the importance of the complementary feeding period for the prevention of stunting :
"Suboptimum complementary feeding is clearly a determinant of stunting, and improvements in most settings need to focus on both feeding frequency and energy density, and ensure an adequate, quality diet, including sufficient micronutrients.”
(Black et al. 2008)
In addition to having detrimental health effects, stunting impacts cognitive development and school performance. Since stunting is a result of chronic malnutrition, it is closely related with other socioeconomic factors. Figure 11 shows how stunting is related to other socioeconomic factors and developmental outcomes.
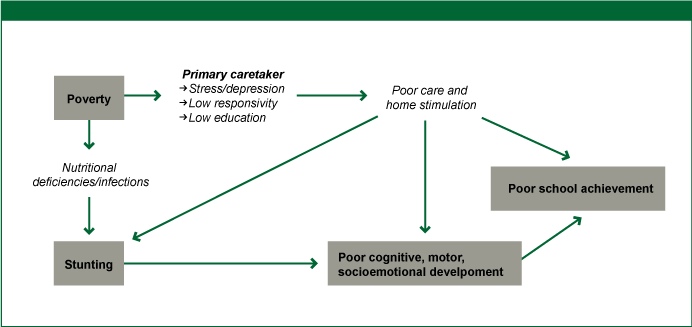
Figure 11: Stunting, Causal Factors and Developmental Outcomes
Source: Grantham-McGregor 2007, reprinted from The Lancet with permission from Elsevier