Lesson 5: Lipids
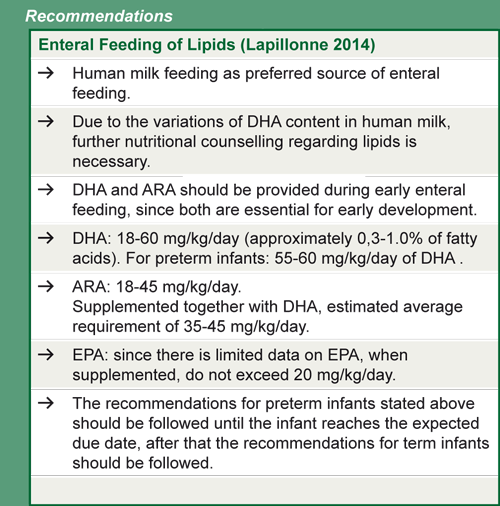
5.2 Enteral requirements
In human milk, fat provides 40 to 55% of the total energy with an average fat content of approximately 3.8 g/100 ml. However, human milk content is highly variable, depending on gestational age, location, maternal diet, etc. Although milk fat concentration increases with the duration of lactation, small differences between term milk and preterm milk are seen in the total content of fat. Triglycerides are the major fat component in human milk (98%), followed by phospholipids (0.7%) and cholesterol (0.5%) (Lapillonne 2014).
In preterm infants, malabsorption of enterally-provided lipids (from human milk or preterm infant formulas) is frequent, due to low levels of digestive enzymes and low concentrations of bile salts in the intestinal lumen (Lapillonne 2014). As much as 20-30% of the fat ingested by preterm infants may be excreted in their stools (Lindquist & Hernell 2010). In addition, pasteurization (62.5°C for 30 minutes) of donor human milk seems to activate the milk bile-salt-stimulate lipase (BSSL) and to change the structure of the milk fat globules leading to further reduction in fat absorption.
Long-chain saturated fatty acids, such as palmitic acid, are present in high amounts in human milk at the sn-2 position of triglycerides (Figure 4):
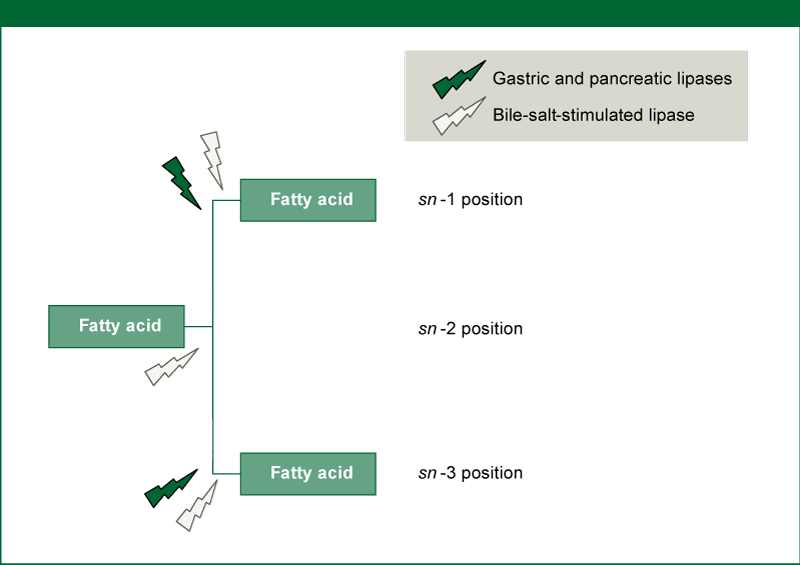
Figure 4: Enzymatic Hydrolysis of dietary triglycerides
(Stereospecificity and chain lengths of fatty acids at the sn- 1, sn- 2 and sn- 3 positions in triglycerides
determine the metabolic fate of dietary fat during digestion and absorption. The enzymatic
hydrolysis of dietary triglycerides is a major activity of digestion, largely occurring in the duodenum.
Preferential hydrolysis by pancreatic and lipoprotein lipases target the fatty acids in the sn- 1 and sn-
3 positions resulting in two free fatty acids and one sn- 2 monoglyceride which has a water solubility
and is absorbed well. In human milk, palmitic acid and myristic acid are found in high proportions at
the sn- 2 position of triglycerides and is therefore well absorbed. The BSSL has no stereospecificity
and equally cleaves the three fatty acids from the triglyceride)
Source: Lapillonne 2014, reprinted with permission of S. Karger AG, Switzerland
Arachidonic acid (ARA)
The sn-2 position of the palmitic acid in human milk, leads to a higher fat and calcium absorption. In preterm infants, the use of synthetic ß-palmitate, has shown to increase fat and mineral absorption and could be responsible for theoretical effects on growth and immunomodulation (Carnielli et al. 1995).
The coefficient of fat absorption is lower with longer-chain fatty acids. Therefore, some preterm formulas have been formulated to include high levels of medium-chain triglycerides (MCT's) (Lindquist & Hernell 2010). Although MCT's tend to be absorbed at a higher rate, no difference was seen in short-term growth parameters in infants when comparing the use of high and low MCT preterm infant formulas (Klenoff-Brumberg & Genen 2003). Further discussion on preterm infant formulas can be found on unit 3 of this module.The fetal brain grows rapidly during the last trimester of gestation. Long-chain polyunsaturated fatty acids (LC-PUFA's) are required for this growth. In utero, small amounts of the essential fatty acids (EFA's) alpha-linolenic acid (ALA) linoleic acid (LA) and much higher amounts of their derivatives, the LC-PUFAs docosahexaenoic acid (DHA, omega-3) and arachidonic acid (ARA, omega-6), are transferred from mother to fetus across the placenta (Lapillonne 2014)(Figure 5):
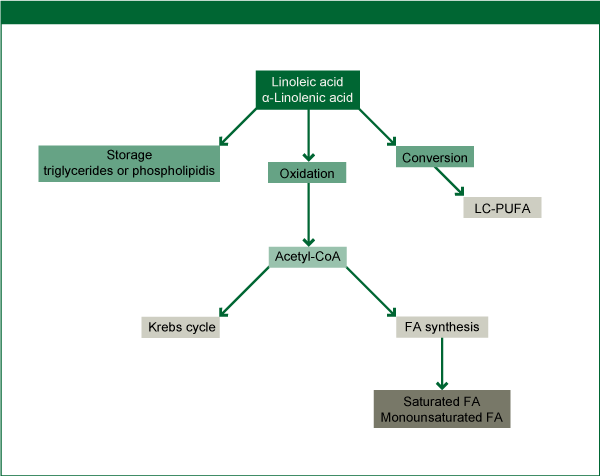
Figure 5: Metabolic pathways of the essential fatty acids, linoleic acid and alpha-linolenic acid
Source: Lapillonne 2014, reprinted with permission of S. Karger AG, Switzerland
LC-PUFA's are provided after birth, by human milk or modern preterm infant formula. In the preterm infant, an EFA deficiency can develop within days of birth, especially when a continuous glucose infusion is given in the absence of parenteral or enteral administration of EFA. The glucose stimulates insulin secretion and blocks lipolysis and hence utilization of body EFA stores. Providing the essential fatty acid precursors ALA and LA to preterm infants is not sufficient: DHA and probably also ARA need to be considered conditionally essential nutrients and given directly to the preterm infant to maintain plasma and tissue levels. Although preterm infants are able to synthesize DHA and ARA from ALA and LA, this endogenous synthesis does not appear to result in LC-PUFA accretion rates equivalent to those found in fetuses of comparable gestational age (Lapillonne 2014).
LC-PUFA's are important for brain and visual development. There are measurable differences in visual acuity (Smithers et al. 2008) and some developmental scores (Makrides et al. 2009) among preterm infants who receive a high dose of dietary DHA. In a randomized controlled trial with 657 infants born at less than 33 weeks' gestation, Makrides and colleagues found that a diet consumed from birth till their due date in which DHA comprised 1% vs. 0.3% of the total fatty acids significantly increased the Bayley Mental Development Index (MDI) scores of girls at 18 months and was associated with higher MDI scores in infants with a birthweight <1250g. Secondary beneficial outcomes of this study were a lower oxygen requirement at 36 weeks and slightly increased length at 18 months' corrected age in the infants consuming the high-dose DHA diet (Makrides et al. 2009). However, the same group has made a follow up at 7-years CA of the randomized controlled trial to determine if the improvements detected at 18 months CA were still present in early childhood. They found that
"enteral DHA supplementation did not benefit IQ, attention, executive function, behavior, visual-spatial perceptual skills, educational progress and quality of life at 7 years´CA compared with a standard-DHA diet.”
(Collins et al. 2015).
The benefits of higher DHA intakes on MDI scores generally appears to be dose-related, as demonstrated in Figure 6, and may be most pronounced in the smallest preterm infants (Lapillonne 2014).
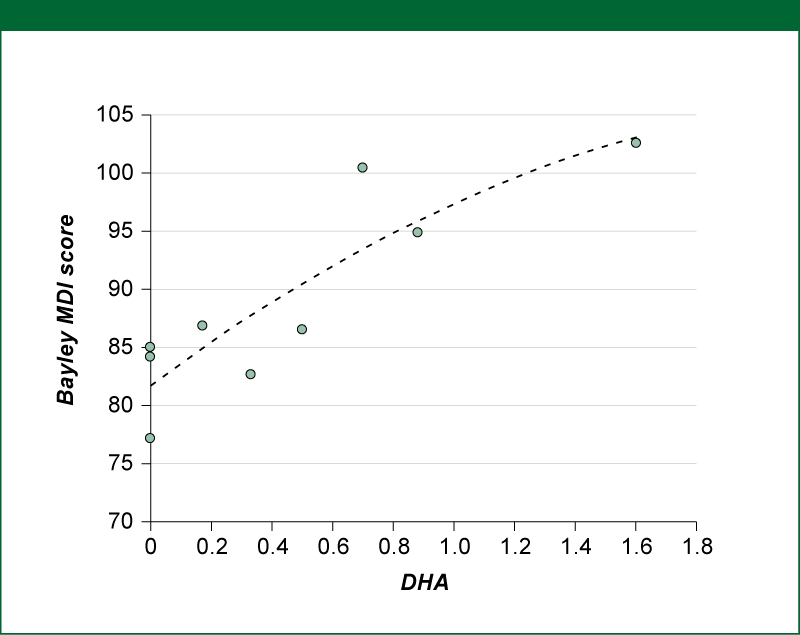
Figure 6: Relationship of DHA intake (expressed as % of total fatty acid in milk during hospitalization) and Bayley MDI Score at 18-20 months' corrected age of preterm infants
Source: Lapillonne 2014, reprinted with permission of S. Karger AG, Switzerland
(adapted from Straarup et al. 2006, Atwell et al. 2013, dit Trolli et al. 2012)