Lesson 2: Practical Management of Infant Feedings
2.1 Parenteral Nutrition
Parenteral nutrition (PN) is given to infants who are unable to meet their nutritional requirements through enteral feeds. PN is considered standard care for most (extremely) premature infants during the first days after birth. Moreover, infants with gastrointestinal malfunction secondary to diseases such as NEC will also need PN until such conditions are resolved (Embleton & Simmer 2014).
When deciding for the use or not of parenteral nutrition, clinical judgment is required to balance its risks and benefits (Table 1).
Table 1: Selected risks and benefits of parenteral nutrition
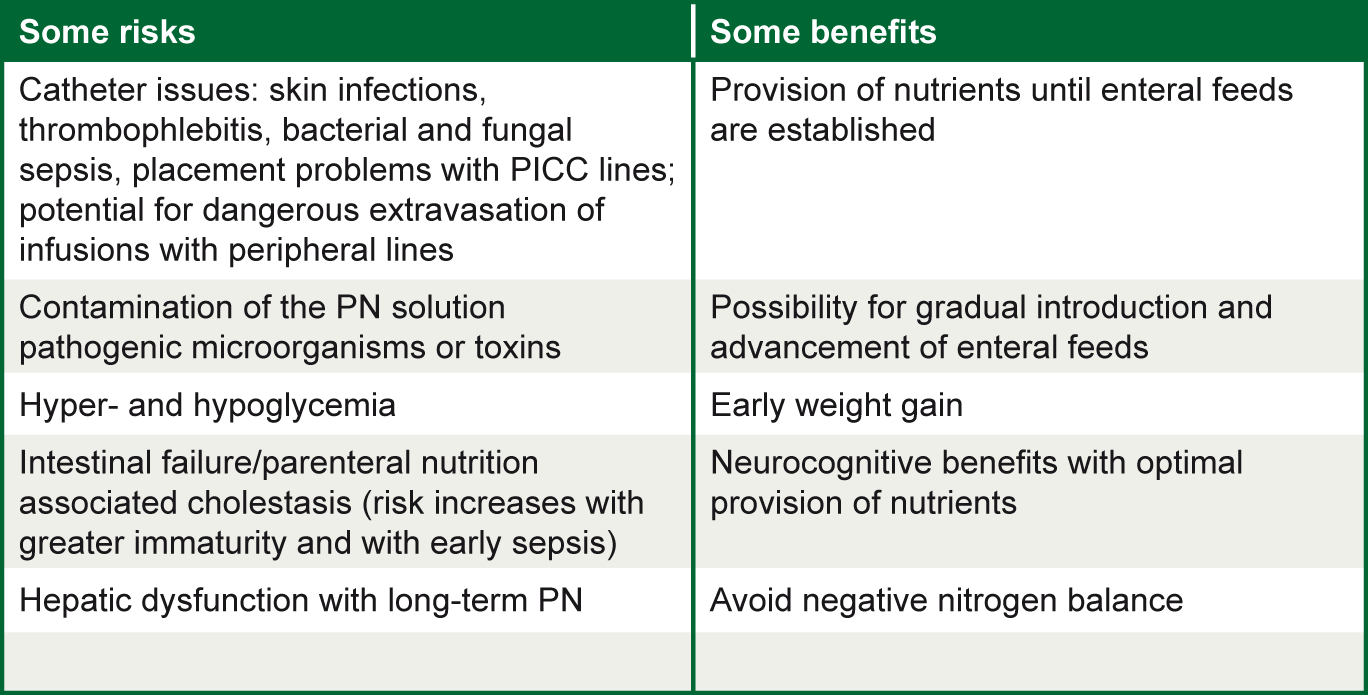
Source: ENeA own table. Information from Embleton & Simmer 2014
In most NICUs in developed countries PN is given routinely to infants <30 weeks and/or <1250g birth weight. The "bridging” between PN and full enteral feeding is approximately 1 to 2 weeks (Embleton & Simmer 2014).
In preterm infants who require longer PN (eg. NEC), it is very important to assure adequate micronutrient and vitamin supplementation to avoid deficits.
An appropriate PN strategy should deliver 2-3 g/kg/day of amino acids (Embleton & Simmer 2014). To promote lean mass accretion, approximately 20-25 kcal of non-protein energy per gram of amino acids is necessary, although further investigation is needed to confirm this value of protein-to-energy ratio. As discussed before (Unit 2, lesson 5), lipids are a good source of energy for preterm infants and it is safe to start early in the PN.
PN is normally administered via a central venous catheter, either in the umbilical vein or percutaneously (PICC, peripherally inserted central catheter). Catheters carry a risk of hepatic thrombosis, although it is rare when its insertion is done in the umbilical vein. PICC can also develop localized skin infections and thrombophlebitis. Invasive bacterial and fungal sepsis are also associated with PICCs. The use of peripheral veins for PN administration may avoid many of these complications, however its use is associated with local complications such as extravasation. The risk of phlebitis may be reduced when PN with intravenous lipid PN co-administration is done.
PN Manufacture and Supply
- Central infusion when solutions are hypertonic with high glucose concentration (>12.5-15%);
- PN can either be mixed in the hospital pharmacy or purchased ready-mixed in bags with standard formulations;
- PN solutions have to be prepared under strict conditions of sterility and the whole process carefully monitored;
- PN are normally kept protected from light (to avoid oxygenation reactions in the presence of light);
- Lipid containers are typically protected from light and the use of amber tubing is advised;
- PN is normally supplied in single use containers such as bags, bottles or syringes;
- To reduce microbial contaminations containers should not be punched more than once;
- Medications should not be added to PN containers, it may cause incompatibilities and contamination;
- Vitamin supplementation would be better delivered in lipid emulsions than in the amino acid/dextrose solution, due to better light protection and more predictable deliverable amounts;
- IPN (Individual PN): prepared and prescribed locally every 24 to 48 h; normally not available at the first day after birth;
- SPN (Standard PN; also called "stock” or "starter” PN in some countries): should be available at all times in the NICU, enabling PN initiation within an hour of birth. SPN has a few advantages over IPN: better provision of nutrients, lower chance of administration and prescription errors, lower risk of infection and lower cost (Simmer et al. 2013).
In Lesson 1 of this unit, the value of implementing a standardized feeding guideline was discussed. Existing standards vary and all are based largely on expert opinion. A global panel of experts in the nutritional care of preterm infants (Koletzko et al. 2014a) has underwritten the following recommendations for parenteral nutrition (Table 2):
Table 2. Suggested target intakes of nutrients from PN in the first week
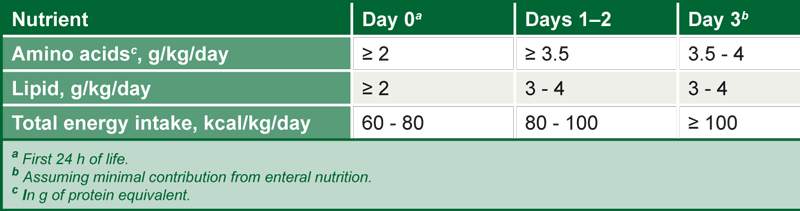
Source: Embleton & Simmer 2014, reprinted with permission of S. Karger AG; Switzerland
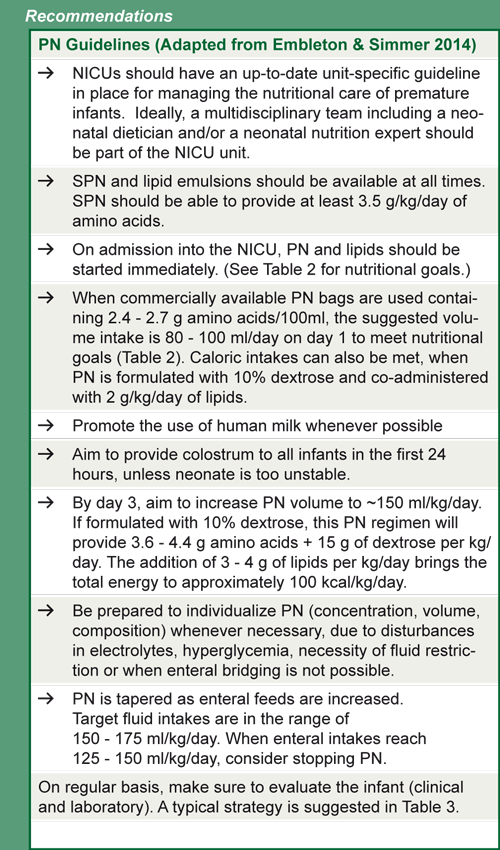
Table 3. Suggested monitoring strategy for PN
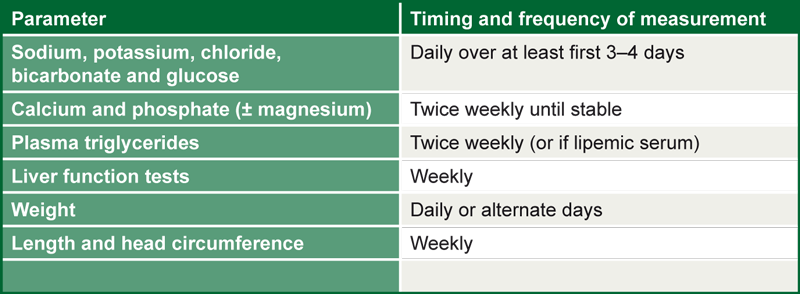
Source: Embleton & Simmer 2014, reprinted with permission of S. Karger AG, Switzerland